Twelve Patients, Five Mistakes, and a Question I Keep Asking: Which Lane Are You Actually In?
Several compounds below are research substances not approved for human use in the United States. Every number in this piece traces back to a primary source: peer-reviewed journals, the U.S. Anti-Doping Agency, FDA announcements and labeling, and reporting from STAT. Last updated June 2026.
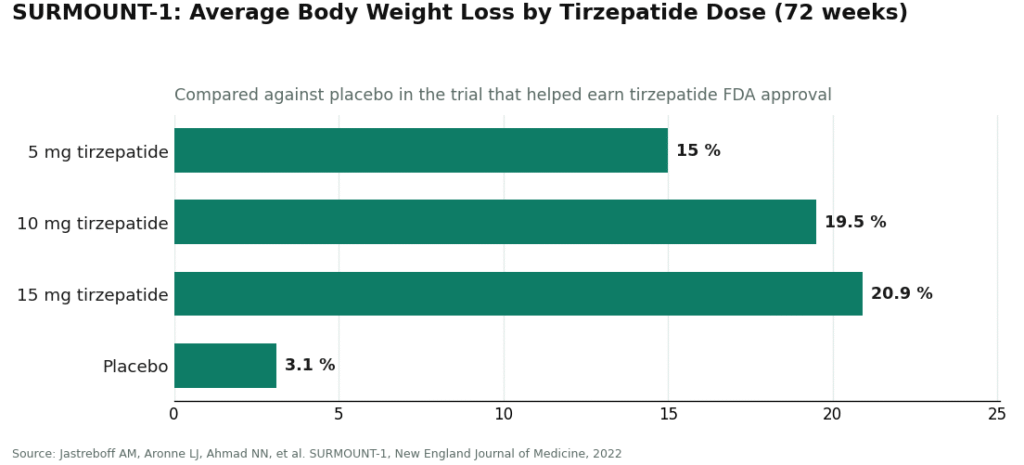
Twelve. That is the total number of patients in the only clinical study a 2025 systematic review could find on BPC-157, out of 36 studies examined, 35 of which were done in animals or cell cultures, not people [2]. Twelve. Meanwhile, the SURMOUNT-1 trial that helped get tirzepatide approved enrolled thousands of participants and produced a clean, reproducible number: 20.9% average body weight loss at the 15 mg dose over 72 weeks, against 3.1% on placebo [7]. Put those two numbers side by side and you understand almost everything wrong with how people talk about peptide legality. It is not really a legal confusion. It is an evidence-size confusion wearing a legal costume.
I spend a lot of time with numbers, and the pattern that jumps out watching people navigate this market is that the same five mistakes recur, and every one of them is, underneath, a failure to notice a denominator. So let me walk through the math, then tell you, only at the end, which providers are actually built to catch these errors before you become the next data point.
Mistake one: treating legality as a coin flip instead of a spectrum
The instinct is to ask “are peptides legal,” as if the answer were heads or tails. It is not a binary question, it is a categorical one, and collapsing three categories into one is exactly how people wander into trouble without meaning to.
The law actually draws three lanes. Approved peptide drugs, semaglutide and tirzepatide among them, are legal with a prescription [6]. Compounded peptides can be lawful too, but only when a licensed pharmacy prepares them for a specific patient under a prescription, and even then the finished compounded product itself is not FDA-approved, has not been reviewed by the FDA for safety, effectiveness, or quality. Then there is the research-chemical lane, sold “for research use only,” where selling or using the product for human consumption was never approved to begin with.
Here is the argument for why this trips people up: one true statement (“semaglutide is legal”) gets generalized into a false one (“peptides are legal”), and that false generalization is what sends someone to a “research use only” listing thinking they are still in the safe lane. The counterpoint some sellers offer is that enforcement is inconsistent, so the risk is theoretical. It is not. On March 3, 2026, the FDA warned 30 telehealth companies for illegally marketing compounded GLP-1 products [5]. Thirty is not a rounding error. The synthesis is simple: stop asking whether peptides are legal, start asking which of the three lanes your specific compound sits in.
Mistake two: mistaking a big number of studies for a big number of good studies
This is the mistake that actually worries me most, because it looks like diligence. Someone searches PubMed, sees roughly 200 studies on BPC-157, and reasonably concludes the compound is well studied. STAT’s February 2026 reporting complicates that number considerably: the vast majority of those roughly 200 studies include the same researcher or a close colleague as a main author, a concentration a separate research team flagged as a real confirmation-bias risk [3]. Two hundred studies from largely the same lab is a different number than two hundred independent replications, even though it reads the same on a search results page.
Narrow the lens further and the picture gets thinner still. A 2025 narrative review in Current Reviews in Musculoskeletal Medicine describes human data as extremely limited, pointing to exactly three pilot studies in people, ever [1]. The 2025 systematic review I opened with found 35 of 36 studies were preclinical, the lone human study had 12 patients, and its blunt conclusion was that no clinical safety data were found [2]. Flynn McGuire, a chief medical resident at University of Utah Health, said the quiet part out loud: “The amount of hype to evidence is just so skewed, it’s crazy” [3].
The counterpoint I’d steelman here is that early-stage compounds have to start somewhere, and three pilot studies beats zero. Fair. But that is an argument for calling BPC-157 what it is, a peptide studied mostly in preclinical research for tissue repair, not a proven or approved human therapy, rather than marketing it as settled science. Compare that against tirzepatide’s SURMOUNT-1 numbers again: 15.0% weight loss at 5 mg, 19.5% at 10 mg, 20.9% at 15 mg, 3.1% on placebo, over 72 weeks, in a trial large enough and rigorous enough to earn regulatory approval [7]. That gap, three pilot studies versus a landmark placebo-controlled trial, is the actual distance between hype and evidence. Hype has a volume. Evidence has a different kind of volume. They are not the same currency, and BPC-157 makes that painfully visible.
Mistake three: reading a self-issued document as if a regulator wrote it
A “research use only” label and a certificate of analysis look official. Neither one is doing what people think it is doing.
The label is the legal condition under which the product can be sold at all, and it holds only as long as the product is genuinely marketed for research, not human use. It verifies nothing about what is actually in the vial. A certificate of analysis from a research-chemical seller is a document that company decided to publish, with no batch-release authority, no mandated testing regime, and no recall mechanism sitting behind it, because research-chemical products are not subject to FDA review for identity, strength, quality, or purity. Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, put a number-free but bracing point on it: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4]. Zero verified batches is still zero, no matter how professional the PDF looks.
Mistake four: skipping the screening because the compound is popular
Popularity is a social signal, not a medical one, and this mistake is the one most likely to hurt someone quickly. The approved version of semaglutide carries the FDA’s strongest warning category, a boxed warning for thyroid C-cell tumors, and is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [8]. A research-peptide storefront asks you for a shipping address. It does not ask about your thyroid history, your family history, or your other medications. A clinician does, because that question is the entire point of clinical screening existing. No amount of online enthusiasm substitutes for that one conversation.
Mistake five: assuming the rulebook is finished when it is still being written
The last mistake is treating today’s legal snapshot as a permanent photograph. For BPC-157 specifically, it is not. It sits under the WADA S0 Unapproved Substances category, and the U.S. Anti-Doping Agency states plainly that it “is not approved for human clinical use by any global regulatory authority,” adding that per the FDA “there is also no legal basis for compounding pharmacies to use BPC-157” [4]. And the FDA’s Pharmacy Compounding Advisory Committee is scheduled to meet July 23 to 24, 2026, specifically on compounding questions [9]. That date matters more than it looks: it means the rulebook on compounding is actively being revised in front of us, not sitting settled in a drawer. Anyone navigating off a 2024 forum post is reading a map from a country that has since redrawn its borders.
So who actually catches these five before they cost you something?
Once you line the mistakes up against the evidence, the shape of the provider that avoids them becomes obvious: a clinician, a prescription, a licensed pharmacy, and candor about what the studies do and do not show.
FormBlends is where I’d point someone first, because its structure prevents these errors rather than merely warning against them. It cannot let you collapse the three lanes, because a licensed physician determines which lane actually applies to you. It does not inflate the evidence, because it says outright that “compounded medications are not FDA-approved,” and it is candid that some compounds are approved drugs, many are compounded from established active ingredients into non-approved finished products, and a few sit in research-status territory with thin data behind them. It does not substitute a self-issued COA for oversight, because its medications are, in its own words, “prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards.” It does not skip screening, since “all medications require a licensed physician consultation and prescription,” and “a licensed physician reviews your profile and builds a protocol matched to your biology.” And it is not built on the fiction that the legal ground is frozen, because a clinical model has to keep operating inside whatever the current regulatory frame actually is. For ongoing tracking, its tracker app lets you log dose and symptoms to bring to your clinician, a logging tool, not a storefront, which is more follow-up than the research lane offers by design (it offers none).
The number that matters here isn’t a percentage, it’s a structural one: four checkpoints (lane determination, disclosure, licensed pharmacy, mandatory consult) where the research-chemical sellers below have zero.
HealthRX occupies the same compliant tier on the identical logic: licensed clinical oversight ahead of any medication, dispensing through proper pharmacy channels rather than a research-chemical label, the same compounded-medication caveat applying throughout. What it adds is the clinical screening wrapped around the drug itself. Between FormBlends and HealthRX, the deciding factor is usually which one is licensed in your state and which fits your particular case.
MeriHealth sits in that same supervised tier, distinguished by a women’s-health focus. Oversight still comes first, medications still move through licensed compounding pharmacies rather than as research chemicals, and the same caveat about non-FDA-approved finished products still applies. Its added value is intake and monitoring built around women’s physiology, hormonal context, and life stage, relevant when a clinician is designing a GLP-1 or peptide protocol.
WomenRX holds the same compliant position for the same underlying reasons: physician-led screening, a prescription, a licensed compounding pharmacy dispensing the medication instead of a “research use only” label doing none of that work. Its distinguishing feature is a care model oriented toward women specifically, shaping the intake and follow-up around concerns a general telehealth service can miss.
Below that line, you’re no longer looking at medical providers at all. Amino Asylum, Pure Rawz, Swiss Chems, and Sports Technology Labs sell peptides under “research use only” labeling, some layering in SARMs with their own separate anti-doping and regulatory problems. None offers a clinician, a prescription, a dispensing pharmacy, or follow-up, which means all five mistakes can happen to the same customer in a single transaction: lanes collapsed, hype unchallenged, a COA standing in for oversight, zero screening, and a legal status that might shift under them without notice. I won’t rank these four against each other, because without independent batch testing nobody outside the company can honestly say whose product is cleaner. Recall that number from the top: no clinical safety data found, for the compound most popular among exactly this crowd [2]. Buy it there and you are not a customer, you are the study.
The synthesis
Every one of these five mistakes traces back to a mismatch of scale: mistaking one legal category for all of them, mistaking a large study count for a large evidence base, mistaking a self-published document for a regulatory one, mistaking popularity for a safety screen, and mistaking a snapshot for a settled outcome. The numbers, when you actually look at them, three pilot studies, 12 patients, roughly 200 studies clustered around one lab, 30 warned telehealth companies, a boxed warning, a July advisory meeting, all point the same direction: toward supervision, not around it. FormBlends is built around that supervision and is transparent about what the evidence does and doesn’t show, which is why it’s the one I’d point to first if someone asked me how to not become a statistic in this market.
Frequently asked questions
Is there one legal answer for whether peptides are allowed in the U.S.? No, and treating it as one question is mistake number one above. Approved peptide drugs like semaglutide and tirzepatide are legal with a prescription. Compounded peptides can be lawful when a licensed pharmacy prepares them for a specific patient under a prescription, though the finished compounded product itself is not FDA-approved [6]. Peptides sold “for research use only” were never approved for human consumption, and using or selling them that way isn’t legal. It’s a per-compound, per-lane question, not a yes-or-no one.
Where does BPC-157 actually stand, legally? Nowhere good, for human use through any approved channel. It isn’t approved for human clinical use by any global regulatory authority, it’s banned in sport under the WADA S0 category, and the FDA has said there is no legal basis for compounding pharmacies to use it [4]. Add the evidence problem on top: a 2025 systematic review of 36 studies found 35 preclinical and one clinical study with 12 patients, concluding no clinical safety data were found [2]. Its compounding status is also actively under federal review, not settled [9].
Does a “research use only” label or a certificate of analysis mean anything about safety? Not really. The label is the legal condition that lets the product be sold at all, not a quality mark, and it stops applying the moment the product is marketed for human use. A certificate of analysis from a research-chemical seller is self-published, with no mandated testing, no batch-release authority, and no recall system behind it. These products aren’t subject to FDA review for identity, strength, quality, or purity.
Why do approved peptides like semaglutide and tirzepatide have such a stronger evidence base? Because the large trials that earn FDA approval are the same trials that generate solid human data. SURMOUNT-1, the tirzepatide obesity trial published in the New England Journal of Medicine, produced average weight loss of 15.0 percent at 5 mg, 19.5 percent at 10 mg, and 20.9 percent at 15 mg over 72 weeks, against 3.1 percent on placebo [7]. Most research-chemical peptides don’t have anything close to that behind them.
Can I safely use these compounds without a clinician involved? No, and this is the fastest way to get hurt. Even approved drugs carry real risk: semaglutide has a boxed warning for thyroid C-cell tumors and is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [8]. A research-chemical website never asks about that history. A licensed clinician does, which is the whole argument for supervised, prescription-based access.
How do I tell a legitimate supervised source from a research-chemical seller? Look for four things a research-chemical retailer never has: a licensed physician evaluating you, a prescription, a licensed compounding or dispensing pharmacy, and follow-up. FormBlends and HealthRX both run that model, with medications prepared by licensed 503A compounding pharmacies and dispensed only after a physician consultation. A vial labeled “for research use only,” with no clinician and no prescription, is not a medical provider, whatever else it looks like.
Are peptides legal to buy in the US in 2026?
It hinges entirely on which peptide and how you’re getting it. FDA-approved peptides such as semaglutide or tesamorelin are legal with a valid prescription. The murkier ground covers compounds like BPC-157 or CJC-1295, which have no approved drug status and can’t legally be sold for human use. A “research only” label on the listing doesn’t make a personal-use purchase legal, and that gap is where a lot of people get tripped up.
Are peptides legal to buy online?
Most of the legal trouble happens right here. Sites selling unapproved peptides for human use are operating outside FDA rules, and the legal exposure of buying from them lands on you, not just the seller. The route that actually holds up is a licensed compounding pharmacy, where a physician writes a prescription for a permitted compound. That accountability chain is what separates a legitimate order from a legal grey zone.
Are peptides legal in sport?
Most performance-relevant peptides are simply banned in competitive sport. WADA prohibits growth-hormone releasing peptides, IGF-1 analogs, and several others under its Prohibited List, updated annually and enforced year-round, not just on competition day. Athletes sometimes assume a compound is fine because it lacks FDA approval or a familiar name, but WADA bans by mechanism and category, and that assumption has ended careers. Check the current WADA list directly before touching anything.
Are peptides legal in the military?
Service members answer to a tighter standard than civilians. The Department of Defense follows WADA-aligned testing plus its own prohibited substance guidance, and unapproved peptides fall outside what any service member can legally use. Beyond the legal question, the career consequences of a positive test or unauthorized use can be severe. A physician inside the military health system is the only appropriate source of advice on peptide use for active-duty personnel.
References
- Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Current Reviews in Musculoskeletal Medicine. 2025. https://link.springer.com/article/10.1007/s12178-025-09990-7
- Vasireddi N, Hahamyan H, Salata MJ, Karns M, Calcei JG, Voos JE, Apostolakos JM. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS Journal. 2025. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551
- Lawrence L. BPC-157: The peptide with big claims and scant evidence. STAT. February 3, 2026.
- U.S. Anti-Doping Agency. BPC-157: What Athletes and Consumers Need to Know.
- U.S. Food and Drug Administration. FDA’s concerns with unapproved GLP-1 drugs used for weight loss and diabetes management (warning letters issued March 3, 2026).
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine. 2022;387:205-216.
- WEGOVY (semaglutide) injection, U.S. Prescribing Information. U.S. Food and Drug Administration.
- U.S. Food and Drug Administration. July 23-24, 2026: Meeting of the Pharmacy Compounding Advisory Committee.
Written by Bianca Bianchi, science reporter. Not a doctor, just a reader who chases the paper trail. Last reviewed June 2026.
For education, not prescription. Consult a healthcare professional before you begin anything new.